






Closure of skin incisions and excisions
Closure of surgical incisions and excisions typically involves placement of deep subcuticular sutures to draw the wound walls together followed closing the wound surface using superficial sutures. The superficial sutures elicit an inflammatory response and frequently produce “railroad track” scarring. Inflammation has also been implicated in the development of hypertrophic and keloid scars. In a study in porcine skin, PTB did not shown adverse responses and excisions closed with PTB healed well (4).
In a pilot clinical study, we compared PTB with standard sutures for superficial closure of wounds produced by removal of skin cancers or atypical nevi (Sandy Tsao, MD; Department of Dermatology, Massachusetts General Hospital). After placement of deep sutures, one half of each wound was closed with sutures and one half was closed with PTB. Thirty-one wounds were treated. Two weeks after surgery, the PTB-closed side showed much less inflammation than the suture-closed side (see figure below). After six months, less scarring was observed on the PTB-closed side (manuscript in preparation).
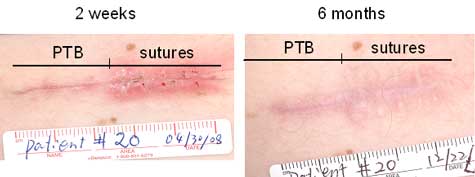 |
| Figure 4. Comparison of healing after epidermal closure of excisional wounds with PTB and standard interrupted sutures, two weeks and six months after surgery. |
Related Publications
4. Kamegaya, Y., W. A. Farinelli, A. V. Vila Echague, H. Akita, J. Gallagher, T. J. Flotte, R. R. Anderson, R. W. Redmond, and I. E. Kochevar (2005) Evaluation of photochemical tissue bonding for closure of skin incisions and excisions. Lasers Surg Med 37, 264-270.
Research Projects
Mechanisms for light activated protein crosslinking
Closure of surgical wounds
Cornea: sealing incisions and transplantation
Peripheral nerve repair
Tendon repair
Blood vessel repair
Neocartilage generation



